Coping With Tinnitus
Strategies, Tips, Tools and Techniques Tinnitus, the medical term for the perception of non-existent noise, often described as ringing in the ear, is a common symptom among vestibular patients and a difficult one to address.
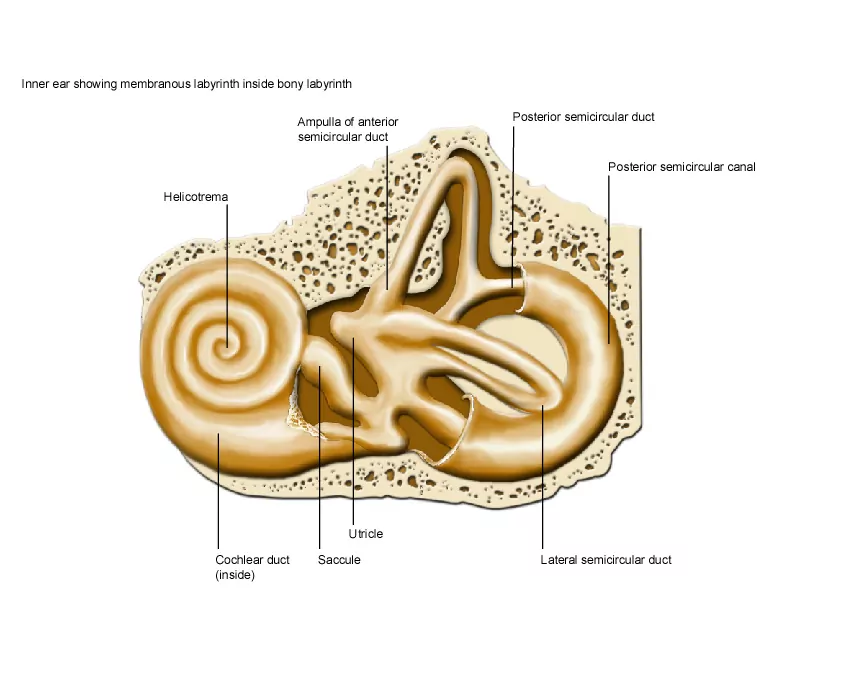
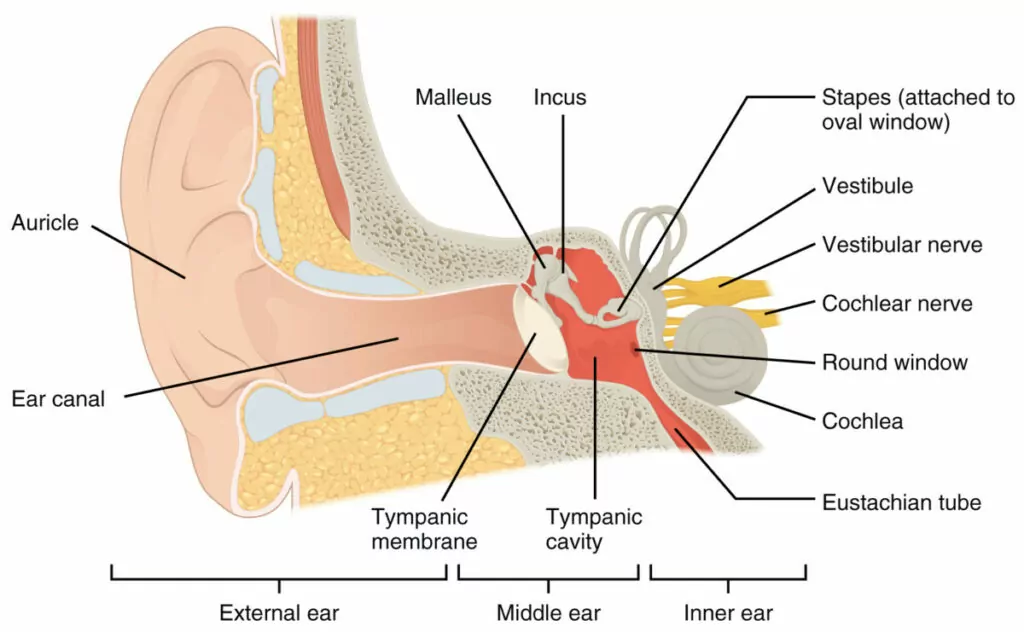
There are three anatomical components to the human ear: the external, middle, and inner ear. The inner ear is a complex system found within a hollow cavity of the temporal bone of the human skull known as the bony labyrinth. In this bony labyrinth, there are several structures responsible for both our sense of hearing as well as our sense of balance and position collectively forming the membranous labyrinth. The bony labyrinth can be thought of as a shell surrounding and protecting the membranous labyrinth. The auditory (hearing) component of the inner ear is driven by the cochlea, a spiral-shaped, fluid-filled organ. The vestibular (balance and position) component of the inner ear is directed by the semicircular ducts, the utricle, and the saccule.
The fluid within the inner ear’s membranous labyrinth is called endolymph (endo-: inside or within). The fluid contained between the bony labyrinth and the membranous labyrinth is perilymph (peri-: around or about). These two fluids contain similar chemicals such as potassium, calcium, sodium, and magnesium, but the concentration of chemicals varies substantially between the two. When the composition of these fluids is disturbed, normal function of hearing and balance may be affected.
Credit: AnatomyTOOL.org
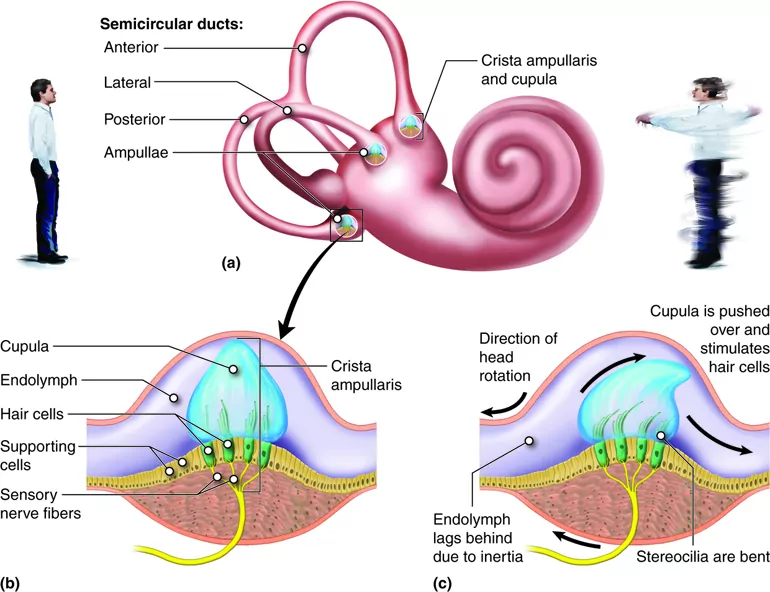
The semicircular ducts are fluid-filled tubes deep within the bony semicircular canals that detect the rotational movement of the head about the axes of motion (X, Y, and Z). There are three semicircular ducts: superior, lateral, and posterior. Each semicircular duct detects the motion of the head around a different axis. The superior semicircular duct detects rotational movement around the frontal, or X, axis (e.g. nodding your head to indicate “yes”). The lateral semicircular duct detects movement around the vertical, or Y, axis (e.g. shaking of the head to indicate “no”). The posterior semicircular duct detects movement around the anterior-posterior, or Z, axis (e.g. touching your ear to your shoulder).
Located at the base of each semicircular duct is a widened area referred to as the ampulla. The ampulla contains the cupula and hair cells. The cupula is a gelatinous structure that spans the entire duct, and its motion is coupled to the hair cells. The hair cells are receptor cells that have hairlike projections called hair bundles that extend into the cupula. When the head moves, the endolymph lags behind due to inertia, which creates a fluid wave that collides with the cupula. The deflection of the cupula, and the hair bundles, activates the hair cells which sends a signal to the brain via the vestibular nerve, a branch of the vestibulocochlear nerve (cranial nerve eight).
This is how the semicircular ducts detect and transmit rotational movement information to the central nervous system to maintain balance and position. In addition, this information is used by our brain to carry out corresponding eye movements as our head turns to maintain forward vision. Each ear has a matching set of semicircular ducts and canals, and they work in tandem. Vestibular symptoms (e.g. dizziness, vertigo, imbalance, etc.) may be seen in semicircular duct disturbances such as benign paroxysmal positional vertigo (BPPV), superior canal dehiscence syndrome (SCDS), and alcohol positional nystagmus.
Credit: AnatomyTOOL.org
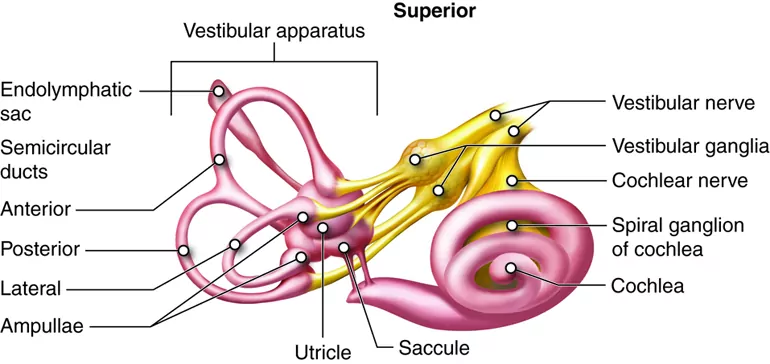
The utricle and the saccule are involved with linear motion of the head. These two membranous structures, referred to as the otolithic organs, are the sole residents of the vestibule, a hollow cavity located between the cochlea and the semicircular canals. The utricle detects linear motion in the horizontal plane (e.g. accelerating/decelerating in a car) and the saccule detects linear motion in the vertical plane (e.g. movement in an elevator).
The otolithic organs each contain a single curved structure called the macula that contains receptor cells known as hair cells and additional supporting cells. Similar to the mechanism of the semicircular ducts, these hair cells contain tiny hairlike projections. These projections extend into a gelatinous membrane called the otolithic membrane. Resting on top of this membrane are microscopic crystals made of calcium carbonate called otoconia. These are commonly referred to as “ear rocks” or “ear stones.” Upon linear motions of the head, these tiny crystals will drag along the otolithic membrane and deflect the hairlike projections of the hair cell. This deflection allows the hair cells of the otolithic membranes to fire off a signal to the vestibular nerve and communicate with the brain that the head is moving in the horizontal and/or vertical plane.
Dysfunctions of the otolithic organs may lead to vestibular disorders such as BPPV or persistent postural-perceptual dizziness (PPPD).

Credit: AnatomyTOOL.org
The endolymphatic sac is a pouch that connects to the vestibule via the endolymphatic duct. The endolymphatic sac is believed to maintain the volume and composition of endolymph as it circulates through the inner ear. If this regulatory system is disrupted, endolymph may accumulate within the inner ear resulting in a condition known as endolymphatic hydrops. In this condition, the excessive volumes of endolymph cause the structures containing endolymph to swell up and may result in vestibular and/or auditory symptoms. Disruption of the endolymphatic sac is only one potential cause of endolymphatic hydrops. Commonly, this condition is associated with Ménière's disease.
Credit: AnatomyTOOL.org
The oval window is a kidney-shaped opening connecting the middle ear to the inner ear and this opening is covered with connective tissue. The footplate of the stapes, one of the middle ear bones, sits on top of the connective tissue. The function of the oval window is to transmit vibrations from the stapes to the inner ear fluid, sending a fluid wave through the cochlea and generating sound through specialized cells. Although its role is primarily related to the auditory system, compromise of the oval window’s seal may result in vestibular problems. A perilymphatic fistula is an abnormal connection between the perilymph-filled inner ear and the middle ear. This undesirable communication between the inner and middle ear may change the perilymph composition and volume which can lead to vestibular and auditory symptoms.
The round window is another connective tissue-covered opening between the middle and inner ear. This membrane is on the receiving end of the fluid wave generated by the oval window. When the oval window bulges inward towards the inner ear, the round window bulges outwards towards the middle ear. Like the oval window, disruption of the round window’s connective tissue membrane can result in a perilymphatic fistula.
Authors: Brian Keith BS, Habib Rizk MD
Affiliations: Department of Otolaryngology – Head and Neck Surgery, Medical University of South Carolina, 171 Ashley Avenue, Charleston, SC 29425

Are you tired of searching for the latest vestibular news? Then sign up for VeDA's free monthly newsletter! V-News includes information on current research, patient stories, VeDA events, and more! It's easy to subscribe, and just as easy to unsubscribe.
Give it a try!
